Crown, the term referring to the restoration of teeth using materials that are fabricated through indirect methods and later cemented into place, plays a vital role in dental care. A crown is designed to cap or entirely cover a tooth, restoring both its function and appearance. In Cornwall, you can trust the skilled hands of Dr. Alma Iancau at Dentistry @ Cornwall to provide you with top-notch crown and bridge solutions. To schedule an appointment, call us at (613) 933-0030 or visit our conveniently located office at 1232 Brookdale Avenue, Unit D, Cornwall.
The main advantages of the indirect method of tooth restoration include:
Indirect restorations using these materials typically exhibit superior mechanical properties compared to those employed in direct tooth restoration, ensuring a higher-quality restoration for your teeth.
With advancements in technology and material chemistry, computers are increasingly integrated into crown and bridge fabrication processes, especially through CAD/CAM technology.
When dental decay is initially detected, Dr. Alma Iancau usually opts for an intracoronal restoration, commonly known as a "cavity filling." These intracoronal restorations come in various materials, including silver-colored amalgam, tooth-colored resin, or gold. Inlays are also considered intracoronal restorations.
However, when a tooth lacks sufficient solid structure due to decay or fractures, it may require an extracoronal restoration. Such restorations, including different types of crowns and onlays, can be crafted from materials like gold, ceramics, or combinations of both.
The choice of restoration depends on several factors, including the remaining tooth structure, aesthetics, tooth position in the dental arch, and the functional forces the restored tooth will face. Dr. Alma Iancau carefully evaluates these factors to determine the best treatment approach.
Restoring a tooth isn't always straightforward. Crowns offer several advantages over extensive pin-supported amalgam or composite restorations. They provide enhanced protection against future fractures and recurrent decay. Indirect crown fabrication techniques result in precisely adapted tooth-restoration margins, ensuring a better seal against decay-causing bacteria present in saliva.
There are various situations where crown restoration is the ideal choice:
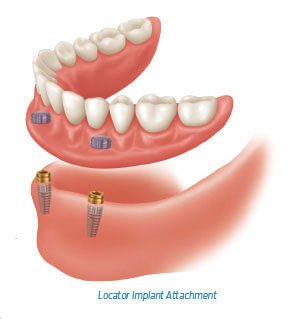
Dental implants are an effective solution for partial or complete edentulism in Cornwall. Once integrated into the jawbone, implants can be fitted with crowns or bridges, providing natural-looking and functional replacements for missing teeth.
Endodontic treatment, also known as root canal therapy, can leave teeth devitalized and vulnerable to fracture. Crown placement following root canal treatment is crucial, especially for posterior teeth that endure significant biting forces. Properly crowned teeth are better protected against fracture and reinvasion by bacteria.
A surveyed crown is an excellent choice when a tooth needs to serve as an abutment for a removable partial denture but lacks the necessary features for this task. The crown can be modified to accommodate the requirements for denture attachment.
Crowns are often preferred for aesthetic smile makeovers when partial coverage (veneer/laminate) isn't suitable. Crowns can alter the size, shape, or shade of teeth while providing exceptional durability, even for individuals who grind their teeth.
Television makeover shows, such as Extreme Makeover, frequently use crowns due to their ability to produce dramatic results within a short timeframe, avoiding the need for lengthy orthodontic treatments.
To prepare a tooth for a crown, a significant amount of tooth structure must be removed, making it an irreversible procedure. It's essential for Dr. Alma Iancau to carefully evaluate each case to determine the most appropriate treatment plan, considering factors like tooth structure, aesthetics, and long-term prognosis.
Proper tooth preparation for a crown is critical. The enamel must be entirely removed, leaving only dentin for the restoration. The amount of tooth structure removed depends on the restoration material used. For example, a full gold crown requires only 0.5 mm of space, while porcelain additions necessitate an additional 1 mm of tooth reduction, totaling 1.5 mm.
In cases where there isn't enough tooth structure for proper crown retention, a build-up material may be required, such as pin-retained restorations or, in severe cases, a post and core. Tooth preparation procedures should be carefully chosen based on the patient's specific needs.
The prepared tooth must have a specific degree of taper (usually 3 to 5 degrees) to allow for proper placement of the crown. The absence of undercuts on the tooth's surface ensures the restoration can be securely attached. However, excessive taper may compromise the crown's grip. A balanced taper of 6 degrees around the tooth's circumference provides both a secure fit and adequate retention.
The margin, the most coronal position of untouched tooth structure near the gum line, is crucial for crown placement. In aesthetic areas, Dr. Alma Iancau strives to place the margin as apical (towards the root tip) as possible, below the gum line, to enhance aesthetics and ensure proper retention. However, biologic width considerations must be taken into account to prevent complications.
Crown restorations, whether made entirely of metal or featuring porcelain components, offer excellent strength and durability. Unlike direct restorations, crowns can replicate the original tooth's functional dimensions, including cusp heights and slopes, thanks to their precision and resilience.
In some cases, teeth may benefit from 3/4 or 7/8 crowns, which preserve a portion of natural tooth structure while enclosing the rest in restorative material. These restorations are often chosen for specific situations, such as improving aesthetics without compromising strength.
All-ceramic restorations offer excellent aesthetics, making them an ideal choice for visible teeth. However, they may not match the strength and resilience of full gold crowns. When aesthetics are paramount, all-ceramic restorations provide a valuable option.
While no dental restoration lasts forever, crowns can provide lasting benefits with proper care . Maintaining good oral hygiene, regular dental check-ups, and avoiding harmful habits like teeth grinding or biting on hard objects will extend the lifespan of your crown.
Dr. Alma Iancau and the team at Dentistry @ Cornwall are committed to helping you maintain optimal oral health with top-quality crown and bridge solutions in Cornwall. Don't hesitate to contact us at (613) 933-0030 or visit our office at 1232 Brookdale Avenue, Unit D, Cornwall, to discuss your dental needs and schedule an appointment.
Crown restorations are essential for preserving and enhancing the function and aesthetics of teeth. Whether you require a crown for restorative purposes, dental implants, endodontically treated teeth, or smile makeovers, Dr. Alma Iancau and the team at Dentistry @ Cornwall in Cornwall are here to provide you with care and durable, aesthetically pleasing solutions. Contact us today to start your journey to a healthier and more beautiful smile.

Retainer (space maintainer) - Dentist Cornwall